Could My PMS Be PMDD?

PMDD (premenstrual dysphoric disorder) is not just severe PMS. It is a cyclical mood disorder driven by an abnormal brain response to normal hormonal changes and it affects 3–8% of menstruating women, most of whom go undiagnosed for years.1-5
What Is PMDD?
Premenstrual dysphoric disorder, or PMDD, is a condition where the brain responds abnormally to the hormone fluctuations that occur during a normal menstrual cycle.1-3 The key word here is abnormal response not abnormal hormones. Most women with PMDD have hormone levels that fall within a completely typical range. The way the brain and central nervous system reacts is where the real trouble lies.
Symptoms emerge in the luteal phase (the two weeks before your period), intensify as your period approaches, and resolve often quickly once bleeding begins. This cyclical, phase-linked pattern is what sets PMDD apart from other mood disorders.6-7
Key Takeaway: PMDD is a neurobiological disorder of hormone sensitivity, not a disorder of abnormal hormone production.1,6,7
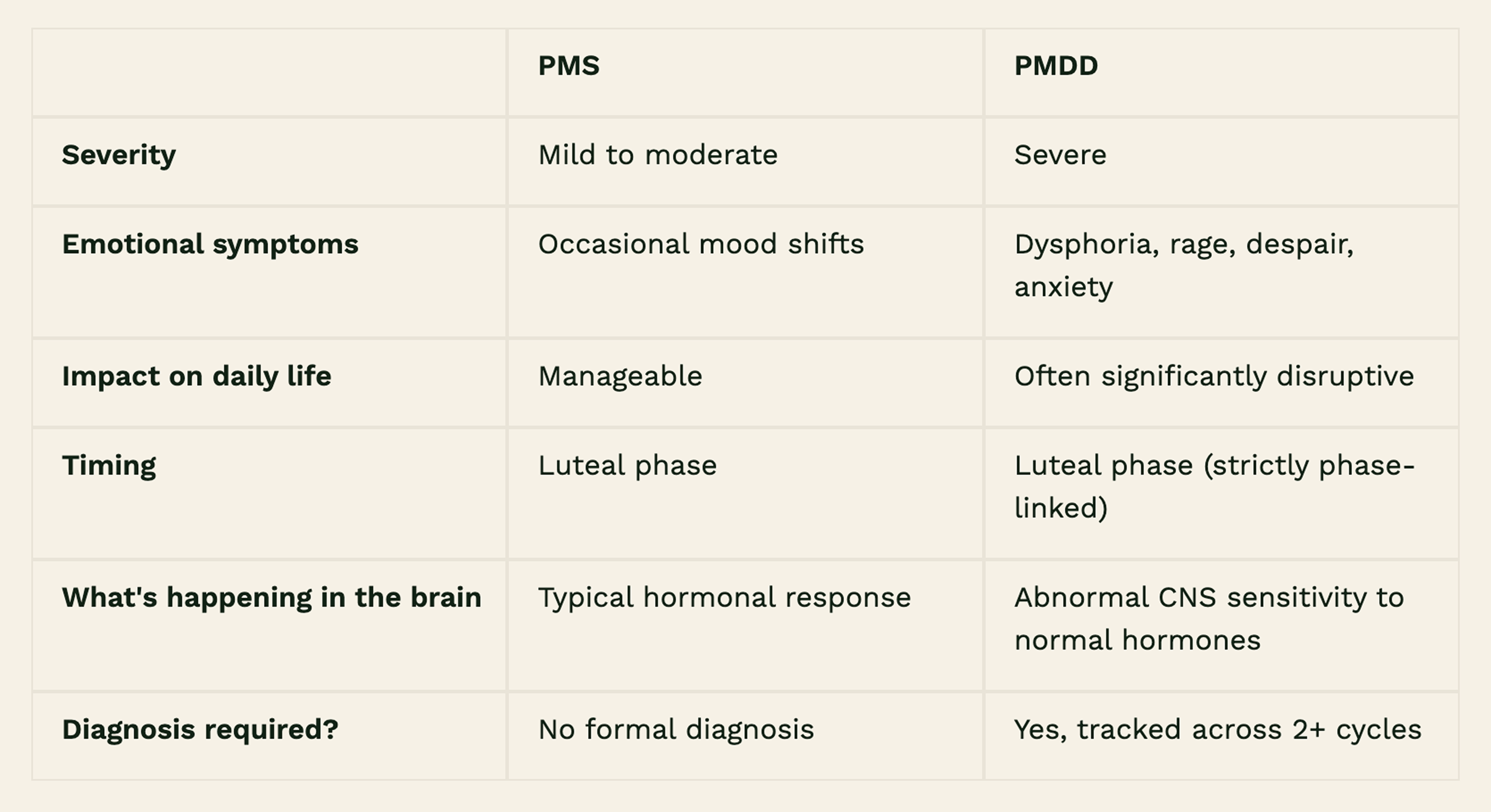
Is It "Just Bad PMS"? Here's the Difference.
This is one of the most common and most damaging misconceptions about PMDD.
PMS (premenstrual syndrome) is real, and it can be extremely uncomfortable. But PMDD is categorically different. Where PMS might look like bloating, breast tenderness, or mild irritability, PMDD involves severe emotional and psychological symptoms that can make it genuinely difficult to function at work, in relationships, and in daily life.
The difference matters because treating PMDD the same way you'd treat PMS doesn't work. PMDD requires a different clinical lens, one that takes the neurobiological and cyclical nature of the disorder seriously.
What Is Happening in Your Body and Brain with PMDD?
Understanding PMDD means looking at brain sensitivity rather than investigating hormones.
Here's a simplified breakdown of what the research shows:
1. The hormones fluctuate normally.
During every menstrual cycle, estrogen and progesterone rise and fall. In women with PMDD, these levels are typically within normal ranges, indistinguishable from women without the condition.1-3
2. The brain responds abnormally.
The central nervous system (CNS) of someone with PMDD appears to have a heightened sensitivity to fluctuations in neurosteroids, particularly allopregnanolone, a progesterone metabolite that normally has a calming effect on the brain.1,6
3. GABA and serotonin signaling are disrupted.
PMDD is linked to dysregulated GABAergic signaling (the brain's primary inhibitory system) and altered serotonin transmission.1,6 These two pathways are central to mood regulation, anxiety, and emotional resilience.
4. The result is phase-linked mood disruption.
Because the sensitivity is tied to hormone fluctuation rather than hormone levels, symptoms track the cycle almost like clockwork. They appear in the luteal phase and lift once hormones drop at the start of menstruation.
Why Is PMDD So Often Missed or Misdiagnosed?
Even though PMDD affects 3–8% of menstruating women, it remains one of the most underdiagnosed conditions in women's health. Why is that?
Symptoms overlap with depression and anxiety. The presentation of PMDD such as low mood, irritability, tension, and dysphoria can look identical to a primary mood disorder if a clinician doesn't ask when the symptoms occur.5,7 If the cyclical, phase-linked nature of PMDD is missed, it becomes easy to misclassify and hard to treat.
Women are often not believed. Symptoms are frequently dismissed as "just hormones" or an inevitable part of being a woman.
There's no single biomarker. Because the issue is one of sensitivity rather than deficiency, standard hormone panels often come back "normal." This can leave women feeling frustrated and without a clear path to diagnosis.
The diagnostic process takes time. A PMDD diagnosis typically requires tracking symptoms prospectively across at least two menstrual cycles. Without that structure, it's easy for the cyclical pattern to go unnoticed.
The downstream consequences of underdiagnosis are serious. PMDD is associated with reduced quality of life, impaired daily functioning, and most critically, an increased risk of suicide attempts.8 This is not a condition to minimize or wait out.
You're Not "Too Sensitive." You Have an Actual Mental Health Diagnosis
If you've spent months or years wondering why your mental health feels tied to your cycle, you are not imagining it. If you've been told it's stress, or anxiety, or just PMS, and that answer has never fully fit, your instinct may be right.
PMDD is a neurobiological condition with a real mechanism, real diagnostic criteria, and real treatment options. Too often, women with PMDD are seen briefly, in a single appointment, outside of the symptomatic phase, by a provider who isn't tracking their cycle alongside their mood. The result is a partial picture and a diagnosis that keeps getting missed.
Where Can You Find Support for PMDD?
PMDD doesn't fit neatly into a 15-minute appointment, and it shouldn't be treated like it does.
1. We take the emotional experience seriously
The irritability, the despair, the sense that you become a different person in the two weeks before your period, these are not character flaws. At July Health, we don't minimize the psychological weight of PMDD or treat it as secondary to the "physical" side of hormonal health. We treat it as what it is: a mood disorder with a hormonal trigger, and one that deserves real therapeutic attention.
2. Therapy is a core part of how we treat PMDD, not an afterthought
Because PMDD involves disrupted emotional regulation at a neurobiological level, therapeutic support isn't just a nice addition to care. It's one of the most evidence-backed interventions available. Working with a therapist who understands the cyclical nature of PMDD, one who can help you build skills for the luteal phase specifically and process the grief and exhaustion that often come with years of being misunderstood can be genuinely life changing. At July Health, therapy is woven into the care model from the start, not referred out as a last resort.
3. We connect the dots between your hormones, your mood, and your history
PMDD doesn't exist in isolation. It frequently overlaps with anxiety, depression, and other conditions and it may intersect with neurodevelopmental profiles like ADHD in ways that make both harder to recognize and treat. Our integrated approach means we're not looking at your cycle in one silo and your mental health in another. We're looking at you as a whole person, with a history, a pattern, and a care plan that reflects both.
July Health offers virtual, multidisciplinary care for women with PMDD across Canada. Our team is here to support you physically, nutritionally, and mentally without dismissal, and without putting your emotional health at the bottom of the list.
Use our easy online booking to book a free consultation with our July Health team today.
July Health is a virtual clinic offering care for women with hormonal conditions including endometriosis, PMOS, PMDD and ADHD. Our team includes Registered Dietitians, Nurse Practitioners, and Registered Social Workers.
References:
1. Hantsoo L, Payne JL. Towards understanding the biology of premenstrual dysphoric disorder: From genes to GABA. Neuroscience & Biobehavioral Reviews. 2023;149:105168. doi:10.1016/j.neubiorev.2023.105168
2. Gupta K, Patel SJ. Prevalence and Management of Premenstrual Dysphoric Disorder (PMDD): Literature Review. rrijm. 2024;9(6):316-321. doi:10.31305/rrijm.2024.v09.n06.038
3. Pataki B, Kiss BL, Juhász I, Kálmán S, Kovács I. Premenstrual dysphoric disorder—an undervalued diagnosis? Preliminary results of a prospective study on Hungarian women. European Psychiatry. 2024;67(S1):S121-S122. doi:10.1192/j.eurpsy.2024.287
4. Lin PC, Long CY, Ko CH, Yen JY. Comorbid Attention Deficit Hyperactivity Disorder in Women with Premenstrual Dysphoric Disorder. Journal of Women’s Health. 2024;33(9):1267-1275. doi:10.1089/jwh.2023.0907
5. Broughton T, Lambert E, Wertz J, Agnew-Blais J. Increased risk of provisional premenstrual dysphoric disorder (PMDD) among females with attention-deficit hyperactivity disorder (ADHD): cross-sectional survey study. The British Journal of Psychiatry. 2025;226(6):410-417. doi:10.1192/bjp.2025.104
6. Schroll J, Lauritsen M. Premenstrual dysphoric disorder: A controversial new diagnosis. Acta Obstetricia et Gynecologica Scandinavica. 2022;101:482-483. doi:10.1111/aogs.14360
7. Islas-Preciado D, Ramos-Lira L, Estrada-Camarena E. Unveiling the burden of premenstrual dysphoric disorder: a narrative review to call for gender perspective and intersectional approaches. Front Psychiatry. 2025;15:1458114. doi:10.3389/fpsyt.2024.1458114
8. Osborn E, Brooks J, O’Brien PMS, Wittkowski A. Suicidality in women with Premenstrual Dysphoric Disorder: a systematic literature review. Arch Womens Ment Health. 2021;24(2):173-184. doi:10.1007/s00737-020-01054-8


