Why Are PCOS/PMOS and ADHD So Hard to Diagnose in Women?

Women with PCOS/PMOS wait an average of two or more years for a diagnosis and women with ADHD face similar delays, largely due to gender bias in medicine.1,2 When both conditions coexist, they can actively mask each other, making diagnosis even harder. July Health is on a mission to shorten this time and improve access to care for Canadian women.
Why Does PCOS/PMOS Take So Long to Diagnose?
Polycystic ovary syndrome (PCOS), recently renamed polyendocrine metabolic ovarian syndrome (PMOS), is one of the most common hormonal conditions affecting women of reproductive age, yet it remains one of the most underdiagnosed. PCOS/PMOS is characterized by hormonal imbalances including elevated androgens (like testosterone) that affect the ovaries, metabolism, mood, and cognitive function.
Despite clear diagnostic criteria existing for decades, the path to a PCOS/PMOS diagnosis is rarely straightforward.
Key stat: In the largest international study of PCOS/PMOS diagnosis experiences, 33.6% of women waited more than two years for a diagnosis, and 47.1% saw three or more healthcare providers before receiving one.1
The barriers aren't random. These patterns are consistent across countries and healthcare systems.
What Does the Diagnostic Experience Look Like for Women With PCOS/PMOS?3
- Dismissed early symptoms: Irregular periods, acne, weight changes, and mood shifts are often minimized or attributed to stress or lifestyle
- Negative clinical encounters: Women report feeling unheard, rushed, or judged
- Caution about treatment: Providers sometimes delay treatment plans even after diagnosis
- Future uncertainty: Concerns about fertility and long-term health go unaddressed
- Self-education and advocacy: Many women diagnose themselves through research before a provider confirms it
Sadly, this diagnostic experience is far too common. In Canada, 34% of women waited more than two years while 41% saw three or more doctors to obtain their diagnosis.4 An astonishing 66% were dissatisfied with the information they received.4 These statistics confirm what we hear from our patients daily: health care providers frequently dismiss their concerns and lack sufficient knowledge of PCOS/PMOS to diagnose it. On average it takes about 2 months to 13 years from the time that a woman starts to experience symptoms to the time that she receives her diagnosis, often due to direct dismissal of symptoms and failure to order diagnostic testing.5
Why Is ADHD Underdiagnosed in Women and Girls?
ADHD in women has been described in the literature as a "hidden diagnosis" and for good reason.6 The condition can often present differently in women, is recognized less by clinicians, and is actively masked by coexisting conditions.6
Key differences in how ADHD presents in women:2,6,7
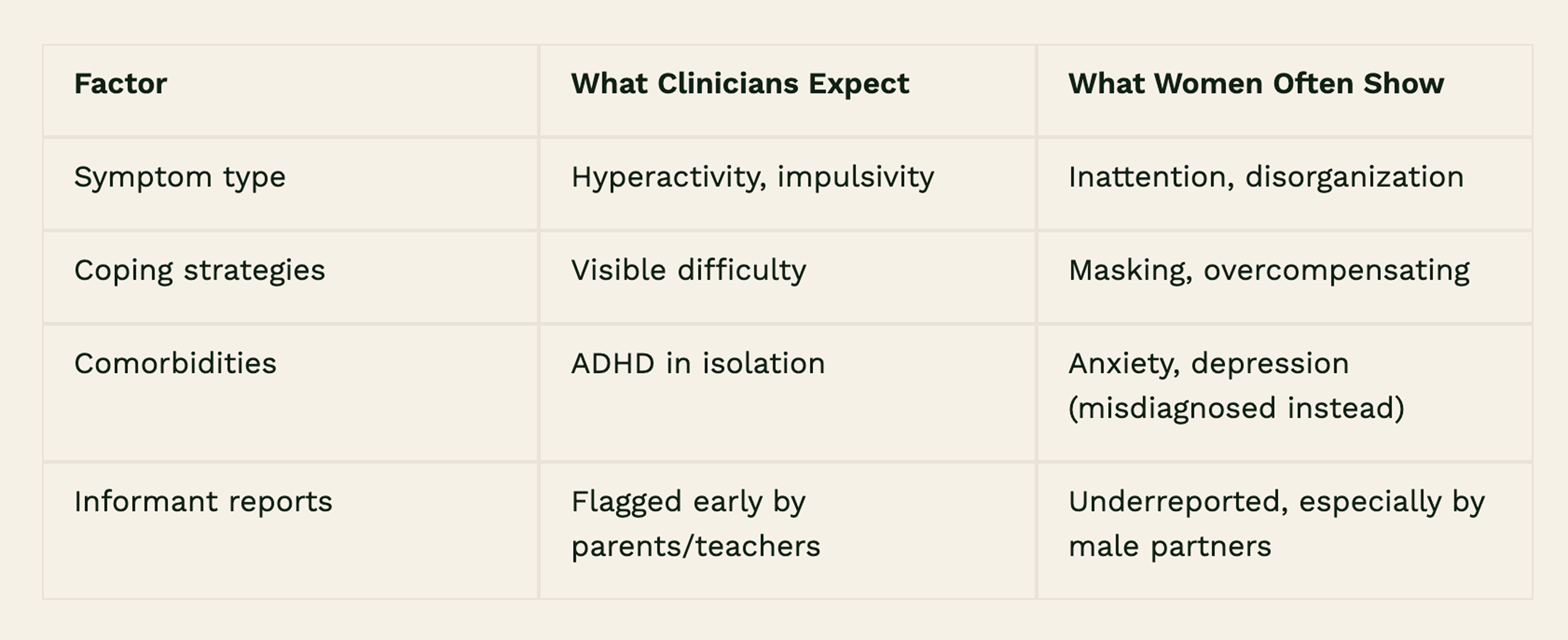
For many women, ADHD stays hidden behind other diagnoses for years. Anxiety gets treated, depression gets treated, and the underlying condition driving both never gets named.2 That's partly because the bias isn't just in one place. It shows up in how clinicians are trained to recognize ADHD, in how the people around a woman describe her behaviour, and in diagnostic criteria that were built on research that largely excluded women to begin with.
Do PCOS and ADHD Mask Each Other?
Here's something the research makes clear, but medicine hasn't acted on yet: PCOS/PMOS affects cognitive function in ways that genuinely resemble ADHD.7-11 Difficulties with focus, organization, and spatial reasoning are measurable and well-documented in women with PCOS/PMOS. But they're almost always chalked up to hormones, or to the anxiety and depression that tend to tag along with the diagnosis, rather than prompting any further investigation.7-11 The only research to directly examine the PCOS/PMOS-ADHD connection found that women with PCOS/PMOS scored notably higher on ADHD symptom scales, particularly around hyperactivity and impulsivity not inattention.2,7,10 That's a meaningful detail: it means the presentation doesn't fit the profile clinicians already struggle to recognize in women, making identification even less likely.2,7,10
What this means in practice is that the symptoms don't get treated, they get blamed on the person experiencing them. Women in this gap often spend years assuming they're lazy, disorganized, or "too emotional," when what's actually happening is two underdiagnosed conditions making each other worse. PCOS/PMOS-driven hormonal changes don't just affect the body. They worsen the exact cognitive and emotional difficulties that an unidentified ADHD diagnosis would explain.
How Should Women Navigate PCOS and ADHD?
If you've been told your brain fog, emotional dysregulation, or difficulty concentrating is "just your hormones," it's worth knowing that the research supports a more complete picture. PCOS/PMOS and ADHD are not mutually exclusive, and one should not be assumed to explain away the symptoms of the other.
The clinical need identified in the literature is clear: bidirectional screening. That means screening for ADHD in women with PCOS/PMOS, and screening for PCOS/PMOS in women presenting with ADHD symptoms. Neither condition should continue to obscure the other.
What Should You Ask Your Healthcare Provider if You Think You Have ADHD?
If you suspect you may have PCOS/PMOS, ADHD, or both, here are questions worth raising at your next appointment:
- "Could my symptoms like brain fog, difficulty focusing, memory issues be related to something else?”
- "Have I been screened for ADHD, or could a referral be appropriate?"
- "If I have PCOS, could hormonal fluctuations be affecting my attention and executive function?"
- "Is there a provider on your team familiar with the overlap between hormonal health and neurodevelopmental conditions?"
Advocating for yourself in a system that hasn't caught up to the research is exhausting but you deserve a diagnosis that accounts for the full picture.
How Can I Get Diagnosed Faster?
If any of this has felt familiar, the years of being brushed off, the diagnoses that never quite fit, the exhaustion of having to fight to be taken seriously, you're not imagining it, and you're not alone. The research is clear that women with PCOS/PMOS and ADHD are systematically underserved by a diagnostic system that wasn't built with them in mind. Getting answers shouldn't take a decade of self-advocacy. You deserve care that looks at the whole picture.
That's exactly why July Health exists. Our nurse practitioners specialize in PCOS/PMOS and can help you get answers faster. Without the years of waiting rooms and dismissed concerns. And because a diagnosis is only the starting point, our dietitians and social workers work alongside you to address the whole picture: the hormonal health, the mental load, and everything in between. You don't have to keep advocating alone.
Book a virtual assessment with our nurse practitioner to get answers faster.
References:


